
If You are Under 60 and Healthy you have More Chance of Dying of a Car Accident than Covid, argues Dr Guy Campbell
We are facing a lethal and unpredictable enemy .Covid 19 is a serious disease. But it’s not the only serious disease, and on the evidence to date, it’s not even the most serious disease…
We are certainly however, facing an unpredictable virus that is impossible to completely eradicate, which means that most of us will at some point be immunised with COVID-19 either from natural spread or potential vaccination. Living with the virus is the new reality.
We need to accept that it is with us and is likely to be here for a long time.
As stated by Professor Lyn Gilbert Infectious Disease Physician: “The virus will likely stay with us and eventually become endemic at a low level, probably another cause of the common cold.”
We need a plan with an end game to stop this present paralysis of fear and one that both minimises lives lost and allows the majority of the population to be able to get on with their lives.
Our leading health experts such as Professor Raina MacIntyre and Professor Bowtell have been widely publicised saying that COVID 19 could kill 130,000 people i.e. 0.5% of the population.

However, on successive Q & As, both their answers to the end game were to continue the policies we have (i.e. suppression/lockdowns) until there is vaccination or elimination. Although hopeful, it would be foolhardy to rely 100% on an unproven immunisation that is up to 2.5 years away according to WHO but at best hope, at least 12-18 months away.
A vaccine is now being rushed through with a potential availability at the beginning of 2021. Our Prime Minister has insisted that it will be mandatory for everyone before facing a public backlash, with the issue opening up considerable ethical and human rights issues.
Although, potentially lifesaving and recommended for the vulnerable and over 70s, it still needs to be voluntary for everyone else. A new vaccine needs more time and research and introduces unknown future risks for uncertain benefit in those who are aged less than 60 and have no health problems. Especially so if the elderly & vulnerable who need the protection have already been immunised.
More interestingly, they blasted Sweden’s approach as the one we must avoid. So, let’s be curious to understand and ask why? And ask what lessons we can learn from their approach.

Sweden is a good comparison as it is similar to Australia in regard to health care and relatively low-density living. Nicholas Lewis’s analysis (reference below) of Sweden’s management of COVID 19 explains why their mortality rates have already plateaued because of possible herd immunity due to both the higher levels of COVID spread and pre-existing partially established T Cell immunity as based on Swedish and German research.
For instance, a study by the Karolinska Institute and Karolinska University Hospital recently found that about 30% of people with mild or asymptomatic COVID showed T-cell- mediated immunity to the virus, even though they tested negative for antibodies. It could be that T cell immunity is the result of a previous infection with common cold coronaviruses and would explain both Sweden’s decline in COVID cases and why 40-87% of all cases are mild, but also because of low T cell immunity, the elderly are so vulnerable.
The current thinking is that herd immunity might be achieved with just 20 per cent of the population infected. Similar evidence for pre covid T cell partial immunity has just come out from The Amazon in Brazil with dramatic decreases in mortality and new cases, potentially due to herd immunity with just 20 per cent of the population infected .

Professor Danny Altmann from the Imperial College in London referred to the research out of Sweden as “robust, impressive and thorough” and stated clearly that “antibody testing alone underestimates immunity. This also would mean that the real case fatality rate is significantly less than what we are told it is by the media. This is of course is very good news from a public health perspective, as it shows that people with negative antibody test results could still be immune to the virus at a cellular level.”
The main argument against this analysis is how long immunity lasts. However, Nobel Prize winner Professor Peter Doherty is strongly convinced reinfection is unlikely, and “even if it was … your prior infection would give you very rapid immunity and you would recover very quickly,” if not then any immunisation will face the same hurdles as natural immunity. Essentially it can be argued that Sweden is coming out of the tunnel as we are barely entering it.
Sweden is not only closer to finishing it’s first and probable only major wave,but if there is a 2nd wave it will be more protected than any of its Nordic neighbours, Australia and New Zealand. So let’s be more practical.

Rather than the projected 130,000 deaths suggested by some of our esteemed professors, Professor Bernard’s Murphy estimation in a Senate inquiry of 14,000 is far more realistic based on UK numbers.
Adrian Esterman, Professor of Biostatistics, University of South Australia further revised this to 10,000 in an Australian model based on Sweden. These morbidity and mortality levels could prove to be much lower in Australia if we can protect Aged Care Facilities from infection. This could and still can be achieved by having small designated care teams working at the homes for 2 weeks on/2 weeks off by Staying overnight at the residences with appropriate Covid testing before attending work. To further increase humanity and kindness, husband’s/wife’s, children, grandchildren & friends could be allowed to see their loved ones if they have been symptom free the previous two weeks with a fresh negative Covid test on the day or the day before the visit. There will never be a perfect system but this seems better than multitudes of part time staff working at multiple centres. Similar precautions could also made for other potential vulnerable populations including our indigenous communities.
We can also improve this figure with a better-prepared health system and improving treatments such as nebulised steroids, remdesivir, potential antibody infusions etc.
So, let’s get more realistic about the figures.
In Sweden in the under 60s, there have been 235 COVID related deaths (approximately 170 had comorbidities) and 5846 deaths overall with an average age of 82. If we extrapolate this to Australia at our 2.5 x greater population, this would equate to 587 deaths in people under 60, and based on Sweden’s figures, 423* would have had comorbidity and 164* would have no comorbidity.
To put this in context, the risk of dying from a brain tumour (497deaths) in under 60s in 2017 according to the Australian Institute of Health and Welfare), is over 3x greater than the projected risk of dying from COVID 19 (164) for previously healthy under 60-year-olds.
The one major assumption is that Sweden is closer to finishing it’s first and probably only major wave as previously explained.
However, if there is a second wave, which is now occurring in Europe it will be more protected than it’s European, Nordic neighbours as well as Australia and New Zealand.
Not least because our natural immune systems are reduced by being in lockdown.
I for one am imploring my patients to exercise, eat healthily, increase their Vitamin D with plenty of outdoor activity, keep connected with others, sleep well and generally being prepared with positive thought, especially if they are fit and well and under the age of 60.
Although for the majority of under 60s Covid will be asymptomatic or mild, for a significant minority there are long term sequelae including respiratory, neurological, cardiac and renal complications with fatigue, shortness of breath and joint pain being the most common prolonged symptoms.
Fortunately as reported at The European Respiratory Society International Virtual Congress “ lung impairment tends to ameliorate over time, which suggests the lungs have a mechanism for repairing themselves”.
Furthermore, promising evidence by Australian Professor Thomas Borody a prominent gastroenterologist, well known for developing triple therapy for H.pylori as quoted in Australian Doctor “international data on prescribing ivermectin for Covid 19 show an almost 100% cure rate”. This and other treatments could well reduce both mortality & morbidity in the future.
For people over 60 and more so for the vulnerable and those over 70, even more awareness and protection is needed, especially social distancing and masks when appropriate, but isolation from loved ones, family and friends isn’t the answer either. There is ample reason to have trust that the precautions being recommended would be followed to minimise risk.
Instead, with lockdowns destroying the livelihood of so many individuals and businesses, we are risking 1,500 extra suicides per year with suicides being 2 ½ times more likely in the UE. This could equate to 4,500 deaths over three years (with a lag lasting two years) as per Professor McGorry’s analysis if UE is at 16%.
Professor Johan Giesecke argues that the correct policy is to protect the old and the frail only – This will eventually lead to herd immunity as a “by-product” – The initial UK response, before the “180 degree U-turn”, was better – The Imperial College paper was “not very good” and he has never seen an unpublished paper have so much policy impact – The paper was very much too pessimistic – Any such models are a dubious basis for public policy anyway – The flattening of the curve is due to the most vulnerable dying first as much as the lockdown – The results will eventually be similar for all countries – Covid-19 is a “mild disease” and similar to the flu, and it was the novelty of the disease that scared people. – The actual fatality rate of Covid-19 is the region of 0.1% – At least 50% of the population of both the UK and Sweden will be shown to have already had the disease when mass antibody testing becomes available
,
However, The Grattan Institute projects 3.4 million Australians will lose jobs. It predicts between 14% and 26 % of the entire Australian workforce will become unemployed as a result of governments’ shutdowns/lockdowns and physical distancing rules. An unemployment rate of 26% could result in an extra 2,450 suicides year, potentially another 7350 deaths over 3 years. On top of this increased mental health illness has resulted in Lifeline 25% up in calls & Beyond Blue 40%, and reports of domestic violence up 23%. Di Farmer Minister of Prevention of Domestic violence recognises this as a “COVID nightmare on the frontline”.
There are also missed and delayed cancers. A UK advisor to Boris Johnson has advised me that “he has heard anecdotally that cancer referrals are down 70% in the UK since the start of the lockdown.” In Victoria, Melbourne’s Peter McCallum cancer centre recorded an almost 30% decline in cancer diagnosis in Stage 3 lockdown alone.
Cardiologists are reporting similar trends in detection of heart disease. Melbourne’s stage four lockdowns will logically expected to be worse. Add to this the fact that 1/3 of GP practices under lockdown are becoming at risk of being financially unviable because patients aren’t seeing their GPs, that Medical Specialists are facing the same issues, and that hospitals are closed, which is delaying most surgeries.
It would be conservative to expect another 5-10% increase in mortalities and morbidity from cancers, heart disease, cardiovascular disease, respiratory disease, diabetes and essentially all other illnesses on top of those from mental health.
At an Australian annual death rate of 160,000+/year this could equate to another 16,000 deaths because of COVID Lockdowns.
In supporting this theory, in the UK The Office for National Statistics advised that an extra 21,000 deaths on top of Covid-19 are attributed to people dying in the home from strokes and heart attacks etc as they were too frightened to go to a hospital, as well as the elderly in nursing homes “giving up’’ amid depressing lockdown conditions. A report in the Financial Times referenced an internal British Government estimate that up to 150,000 people in UK could die prematurely of conditions other than Covid-19 because of lockdown.
Essentially, we are risking a 10-20-fold increase in mortality in those aged under 60 from COVID lockdowns compared to COVID itself. This is on top of the devastation caused to our society due to a collapsed economy with poorer health, education, sports and the arts. Thus, equating to a massive decrease in our standard of life. Furthermore, The UN Secretary General Antonio Guterres has warned that the coronavirus pandemic was becoming a human rights crisis, with authoritarian responses, surveillance, closed borders and other rights abuses.
Who would ever have predicted the arrest and handcuffing of a pregnant woman in front of her two children because she had dared to put up a Facebook post in support of lockdown protests, or the use of surveillance cameras in public parks ,would be happening in Victoria?
We have literally gone from the most liveable city in the world to the most authoritarianism, all under the guise of public health.
In Australia we have had approximately 100,000+ deaths in the last eight months including 803 from Covid 19 — average age well over 80.
By educating the public with these figures of cardiac, respiratory, cancer, mental health and diabetes deaths we can, furthermore, put COVID 19 more into perspective.
Thus, it can be strongly advocated that lockdowns have large non-COVID implications, as well as those on the economic well being of our future generations.
From a GP’s perspective I have multiple elderly patients who are distressed because they have had their basic human rights removed in not being able to see their children, grandchildren or close friends. I have multiple patients awaiting delayed surgery, including a young man requiring urgent lifesaving cardiac surgery.
I also have several younger patients living alone in apartment blocks begging me to do whatever I can to persuade my medical colleagues to advice Government to end this cruel lockdown.
I already have experienced one COVID related suicide and another overdose. I have never before seen so much anxiety, stress and disharmony within our community. Given the large scale decline in our communities mental health, the only ever justification to put healthy populations into such lockdowns should be in localised areas where there is a serious risk of overwhelming the Health System. The intensity of the lockdowns has emerged from a dangerously misplaced perception of humanitarianism, when the reality is that they may do far more damage to peoples lives and wellbeing than the virus itself.
Let’s persuade the other states to learn from the errors made in Victoria.
A, Protect aged and nursing home residences with designated trained staff, and allowing the residents to see their loved ones with preventative precautions. Nothing is crueler than the situation we have now with the most vulnerable dying alone in isolation.
B. To avoid hard lockdowns at all costs unless localised health services are threatened to be overwhelmed. Of course if we continue precautions of social distancing and the wearing of masks, etc when appropriate, and ensuring the safety of residential aged care facilities and vulnerable communities, further hard lockdowns should not be necessary.
Simply, there is plenty of good evidence of the increased risk of suicide, and other health risks that are increased due to lockdown measures. This should be publicised and used to influence the COVID response/lockdown policy.
Government needs to be more honest and open in reporting Covid deaths. For instance the four deaths in the under 50s to date apparently all had comorbidities such as cancer, extreme obesity, heart and lung disease.
Furthermore as reported in The Times “No child who was not already profoundly ill has died of Covid-19 in Britain, a large study has indicated, with the researchers saying that the results should reassure parents as a new school term begins.”

In Australia to date, no healthy person has died under the age of 50 from Covid. Yet the under 50s and especially the under 40s are the most anxious because of the fear being whipped up by politicians and the media.
Let’s Lead by Hope, Not Fear.
Footnote
I have been in touch with The Swedish embassy trying to obtain comorbidity data on their COVID stats and, I have just received this table below “Chances Surviving Covid 19 by Age and Sex” which is based on their
data , and is probably the most accurate we can use to project what to expect in Australia. This further confirms that the risk of mortality in healthy under 60s is less than that of the flu ,in fact the chances for survival for all males under 60 with no underlying health condition is 99.996%. or 99,996/100,000 and for all females 99.9976% or 99,997.6/100,000 which combined equates to 3.2 deaths/100,000.
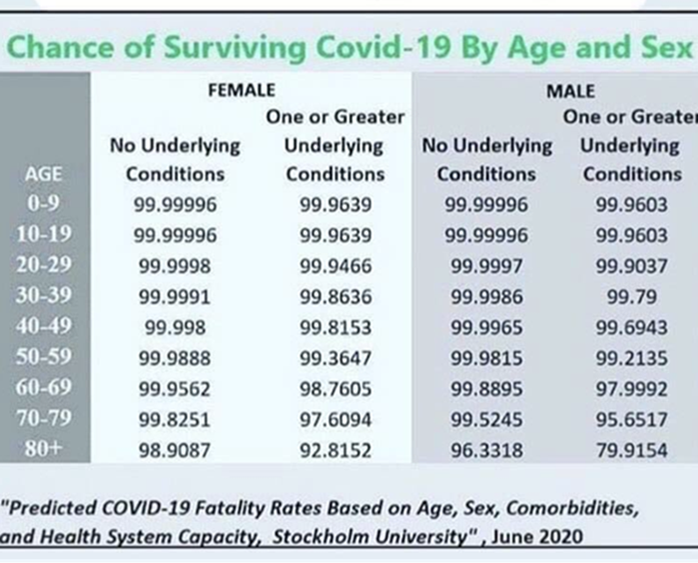
To really put the risk of Covid 19 into perspective for healthy under 60-year-olds, the fatality rate from all car accidents is 5.4/100,000 population per year based on Australian Government statistics with 1182 total fatalities in 2019 with 919 under 64. Based on this, for healthy under 60-year-olds the risk of dying in a car accident is vastly greater than the fatality rate from Covid at 3.2 deaths /100,000, yet it would be deemed as madness to suggest that everyone under the age of 60 shouldn’t be allowed to drive.
Conversely the table shows how lethal the virus is for males with any health condition over the age of 80 with a rate of over 20% mortality.
This is where we need to put our resources and not put whole states or populations into lock down.
Dr Campbell has been a GP for 34 years. He and his team have been recognised by the Australian Primary Care Collaboratives (APCC) for their outstanding results in Diabetes Control. (Best recorded results by any GP in Australia) His previous publications include: “If I Ruled Medicare” published in The Medical Observer.
September 24, 2020 at 10:21 pm
Great reading and positive information Guy.
I agree totally with your views regarding the mismanagement of Covid 19 .
The Government and the Media have created an unnecessary fear amongst our population and in reality, have divided our population and created many other health risks by introducing a mandatory lock down in Victoria !
The increase in Mental Health issues in our community due to Covid lockdown, will prove to be the biggest reason for mortality in the coming years that will affect a great number of Australian families and relatives!
Mental Health issues caused by the Covid lockdown will have long lasting affects throughout our community and this will continue to worsen until we can once again interact with family and friends and resume work!
It is inhumane to prevent people from be able to interact with others!
People are not designed or mentally or physically capable of being isolated !
Keep up the fight and great work Guy ?